The Silent Sentinel: The Rise of IoT and AI-Driven AED Management in 2026
For years, an AED was treated like a quiet safety box on the wall.
A business bought it, mounted it in a hallway, placed a sign above it, and maybe added it to a monthly inspection checklist. After that, everyone hoped it would be ready if the worst happened.
You could call it the “install and hope” approach.
You installed the AED. You hoped the battery was good. You hoped the pads had not expired. You hoped nobody moved it, blocked it, or forgot to check the status light.
That approach may have been common, but it was never ideal. In 2026, it is becoming even harder to justify.
AED management is changing. New connected AED systems, smart cabinets, cloud-based monitoring, emergency registries, and AI-supported feedback are turning AEDs from passive equipment into active parts of a workplace safety plan.
That does not mean every AED is suddenly a robot doctor on the wall. It means businesses now have better tools to answer a basic but important question:
Is our AED actually ready?
The Problem with the Old AED Model
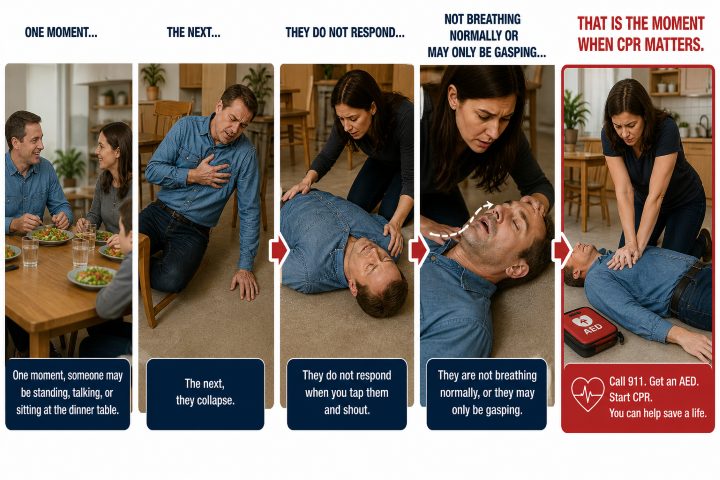
Most AED problems are not dramatic. They are ordinary.
A battery gets weak. Pads expire. A cabinet gets blocked by storage boxes. The AED is moved during remodeling and never returned to its original spot. The person responsible for checking it changes jobs, and the task quietly disappears.
Nobody notices until the emergency happens.
That is the risk with old-school AED management. It depends heavily on people remembering to inspect a device that may sit unused for years, but still has to work perfectly the moment someone collapses.
In a cardiac emergency, those small maintenance details are no longer small. CPR needs to begin quickly. The AED needs to be found quickly. The device needs to turn on, guide the rescuer, analyze the heart rhythm, and deliver a shock if needed.
“I thought someone checked it” is not much of a safety plan.
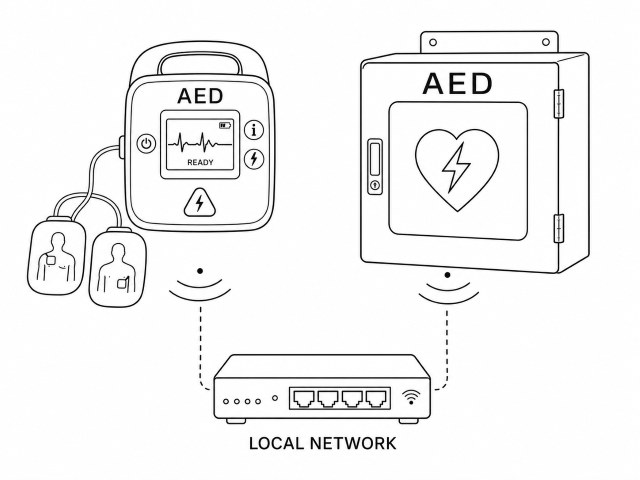
Connected AEDs Make Readiness Easier to Track
IoT stands for Internet of Things. In plain English, it means everyday equipment can connect and send information.
For AEDs, that is a big deal.
A connected AED or smart AED cabinet may be able to report whether the device is ready, whether the battery needs attention, whether the pads are nearing expiration, or whether the cabinet has been opened.
Instead of relying only on a clipboard hanging nearby, the system can send alerts when something needs to be fixed.
For a small office with one AED, that might prevent a missed battery replacement. For a company with several locations, it can make a much bigger difference.
A safety manager can see which AEDs are ready and which ones need attention without calling every building, school, branch, warehouse, or clinic. That kind of visibility matters, especially when one missed inspection can leave a device unavailable at the worst possible time.
The real benefit is simple: AED readiness becomes something you can verify instead of something you assume.
The 2026 Readiness Audit
If your organization has an AED, these are the kinds of questions worth asking before an emergency happens:
- Do we have a digital log or written record of our recent AED checks?
- Do we know when the pads and battery expire?
- Is our AED registered with local dispatch, PulsePoint, or another AED registry if available in our area?
- Who receives an alert if our AED cabinet is opened right now?
- Is the AED easy to find, or is it blocked by furniture, boxes, or locked doors?
- Do employees know who calls 911, who starts CPR, and who brings the AED?
Smart Cabinets Add Another Layer of Protection
The cabinet matters too.
An AED mounted inside a clean, climate-controlled office hallway has a different environment than one placed near a warehouse entrance, school gym, church lobby, manufacturing floor, outdoor recreation area, or busy public building.
Heat, cold, dust, humidity, and foot traffic can all create problems over time.
Some newer AED cabinets can monitor conditions around the device. Depending on the system, they may track temperature, humidity, cabinet access, or whether the AED has been removed.
That may sound like a small upgrade, but it solves a real problem. AED pads and batteries are not meant to be forgotten forever. A device can look fine from the outside while still needing attention inside the case.
Smart cabinets help catch those issues before an emergency exposes them.
AI Can Help During the Emergency
Connected technology can help before the emergency. Artificial intelligence and improved AED feedback can help during the emergency.
This is where the technology gets more interesting, but it should still be explained in practical terms.
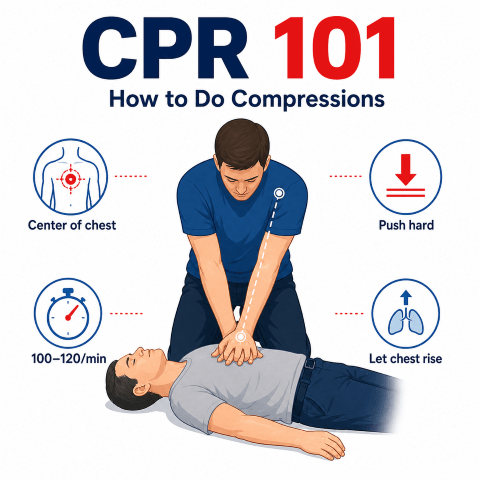
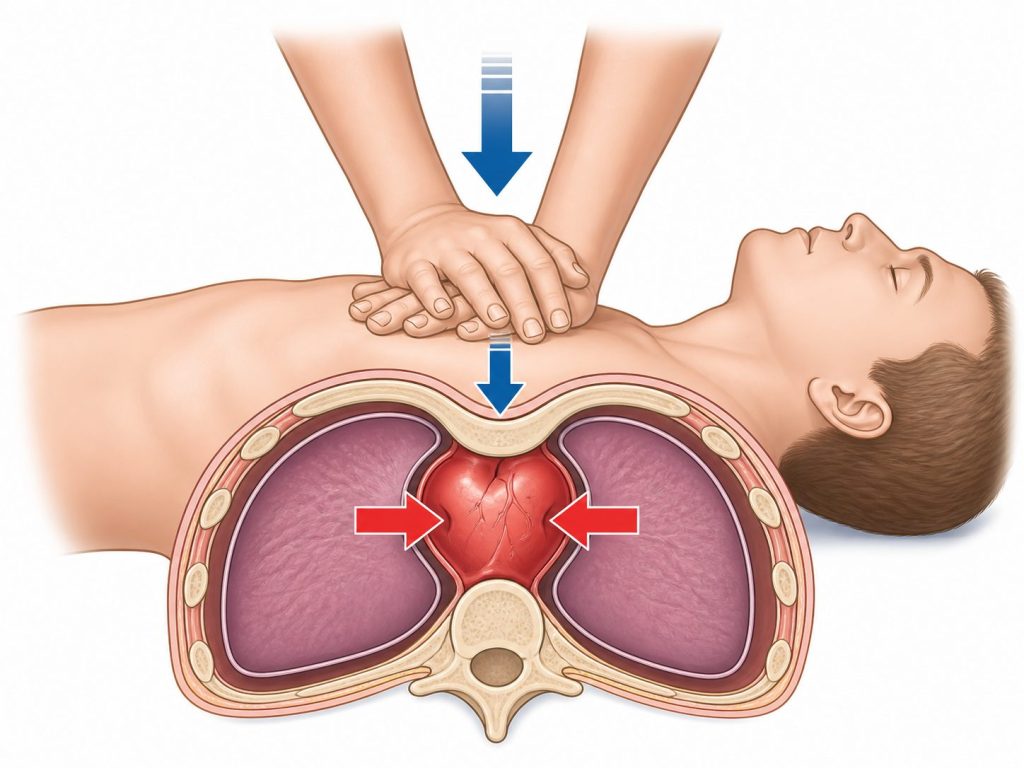
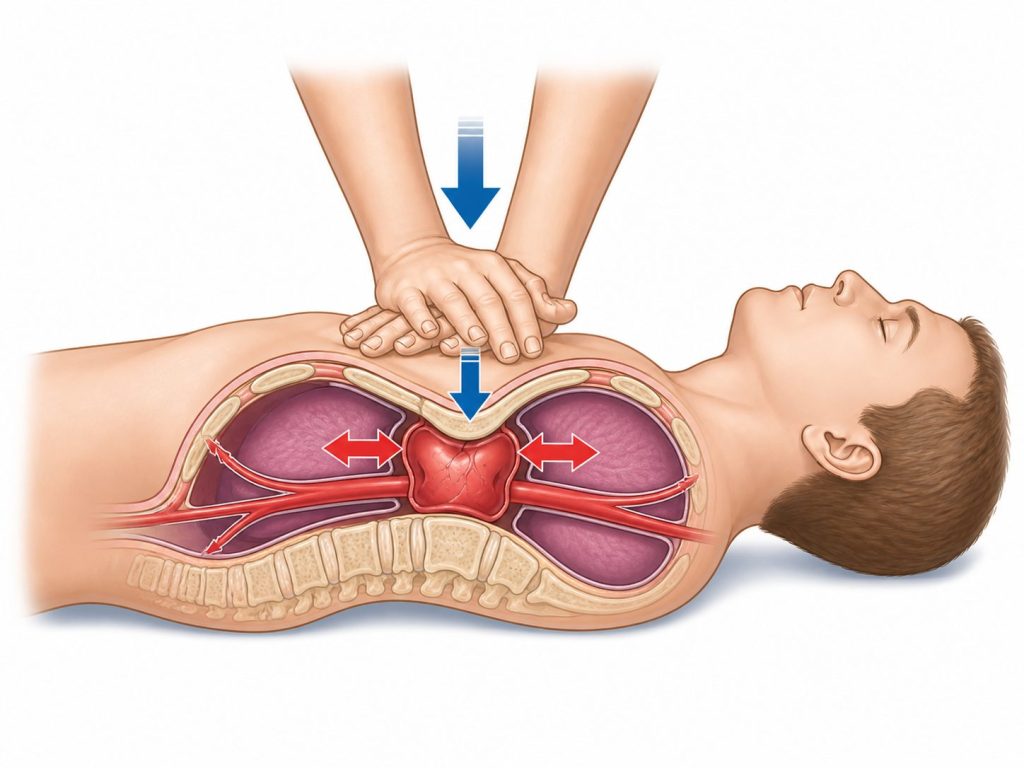
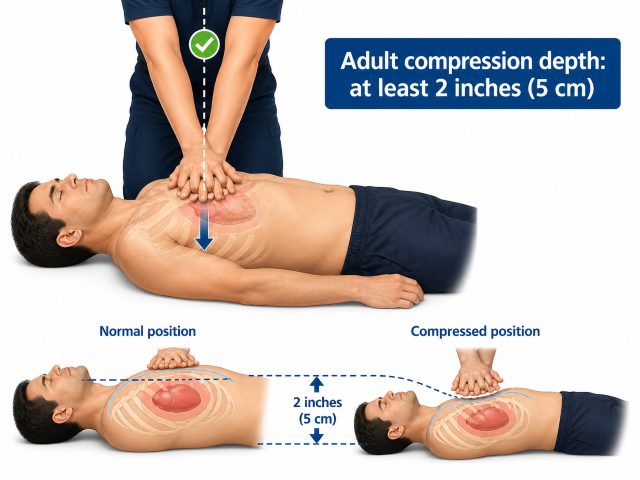
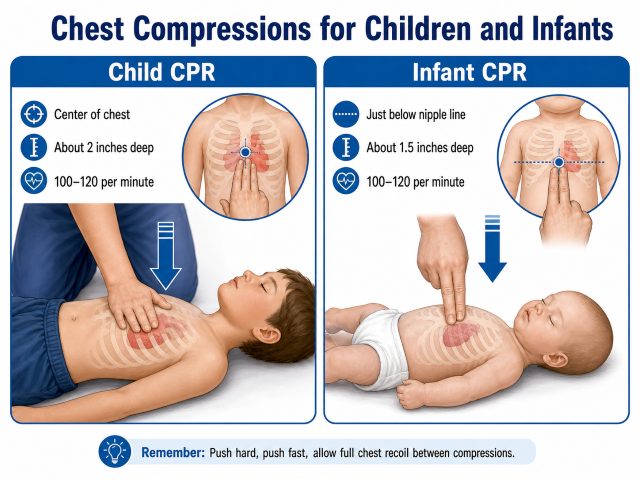
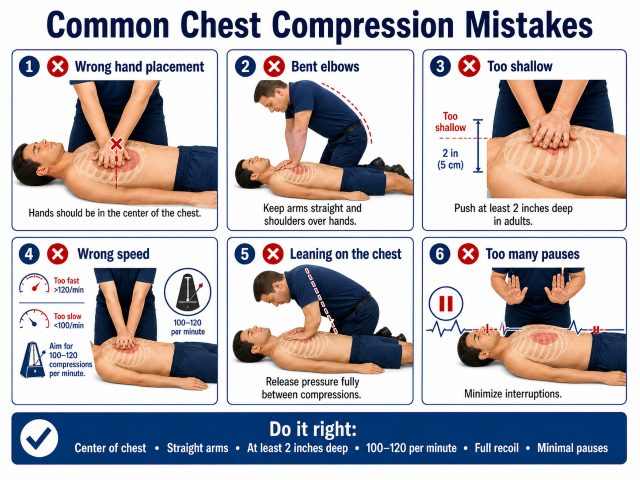
Some newer AEDs and CPR feedback systems can help guide rescuers on compression depth and rate. If the person doing CPR is pressing too shallow, moving too fast, or slowing down, the device may give voice prompts to help improve CPR quality.
That matters because CPR is physically demanding. In a real emergency, people are scared, adrenaline is high, and even trained responders can lose rhythm or pause too long.
AI-supported feedback does not replace CPR training. It gives the rescuer support in the moment.
The best way to think of it is this: training prepares the person, and the device helps coach them while they work.
Reducing Pauses in CPR Matters
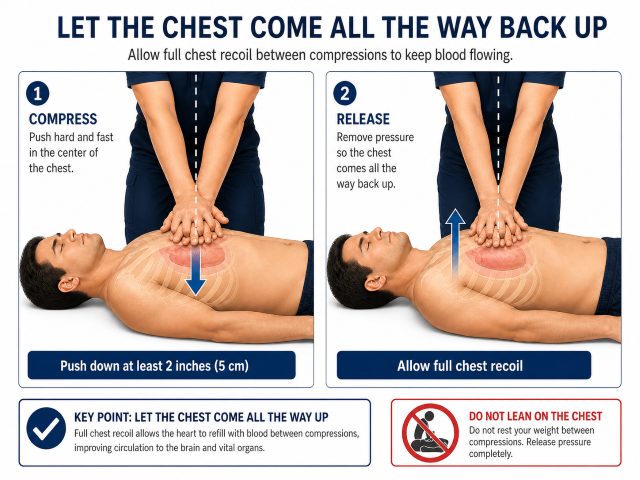
One of the major goals in cardiac arrest response is reducing unnecessary pauses in chest compressions.
Every time compressions stop, blood flow drops. That is why modern CPR training places so much emphasis on keeping compressions going, switching rescuers when needed, and resuming CPR immediately after a shock is delivered.
AED technology continues to improve in this area too. Some systems are designed to reduce interruptions during rhythm analysis and help rescuers stay focused on high-quality CPR.
For employers, the takeaway is not that the AED does everything on its own. It does not.
Someone still has to recognize the emergency, call 911, start compressions, bring the AED, expose the chest, apply the pads, and follow the prompts.
Technology can make the process smoother. Trained people still make the response happen.
AEDs Are Becoming Part of the Larger Emergency Network
One of the biggest changes in AED management is that these devices are becoming more connected to the wider emergency response system.
In the past, a workplace AED often existed only for that building. It might be available to employees, customers, students, patients, or visitors inside the facility, but local emergency responders may not have known it was there.
That is starting to change.
AED registries and emergency response apps can help identify where AEDs are located. In some areas, this can help dispatchers, first responders, or trained community members find the nearest available AED faster.
This matters because cardiac arrest does not politely happen next to the best-prepared person in the building.
It may happen in a parking lot, on a sidewalk, at a youth sports event, in a church fellowship hall, outside a school, or near a neighboring business. If an AED is nearby and ready, it may be useful beyond the four walls of the organization that purchased it.
That is a major shift. A workplace AED is no longer just a private safety item. It can become part of the community’s emergency response network.
Better Data Can Help After the AED Is Used
AED management does not end when the device is opened.
Modern AEDs can collect important event information, such as when the device was turned on, whether a shock was advised, when shocks were delivered, and how the response unfolded.
That information can be useful for EMS documentation, hospital care, internal review, and future training. It can also help leaders understand what went well and what needs improvement.
After a real emergency, people often have questions.
- Did we start CPR quickly enough?
- Did someone call 911 right away?
- Was the AED easy to find?
- Did employees know what to do?
- Were there delays we could prevent next time?
Event data can help answer those questions more clearly.
It can also help support the people who responded. Performing CPR or using an AED in a real emergency is not a small thing. Employees may replay the event in their heads afterward, wondering if they did enough.
A thoughtful post-event review can help them understand what happened, what actions they took, and how their response helped.
Cybersecurity Should Be Part of the Conversation
Any time medical equipment connects to a network, IT departments are going to ask questions. They should.
Connected AED systems may raise concerns about Wi-Fi access, data security, software updates, privacy, and who receives device alerts.
Those are fair questions, especially for schools, healthcare offices, government buildings, large employers, and companies with strict technology policies.
Before choosing a connected AED system, it is worth asking:
- How does the device connect?
- Does it use Wi-Fi, cellular service, or another method?
- What information is being sent?
- Who receives alerts?
- Is the data encrypted?
- What happens if the connection goes down?
- How are updates handled?
- Does the system require access to the company’s internal network?
The point is not to make AED ownership more complicated. It is to make sure the system improves safety without creating unnecessary headaches for IT, compliance, or operations.
A connected AED should make readiness easier to manage, not harder.
The Human Side Still Comes First
Even with smart cabinets, cloud dashboards, AED registries, AI feedback, and better data sharing, the most important part of the response is still human.
- Someone has to notice the emergency.
- Someone has to call 911.
- Someone has to start CPR.
- Someone has to bring the AED.
- Someone has to keep going until EMS arrives.
That is why AED technology and CPR training belong together.
A connected AED can alert you when pads expire. It cannot build confidence in your staff by itself.
AI feedback can coach compressions. It cannot replace hands-on practice.
A registry can show where the AED is located. It cannot guarantee someone will know what to do under pressure.
The strongest safety programs combine reliable equipment with trained people.
That means employees know where the AED is. They know who calls 911. They know how to start compressions. They have practiced with a training AED. They understand that the device will talk them through the steps, but they still need to act.
That confidence usually does not come from reading a policy. It comes from practice.
Moving Beyond “Install and Hope”
In 2026, AED management should not be treated as a one-time purchase.
Buying the AED is the start. Mounting it in a visible place is important. But the real goal is readiness.
That means knowing where your AEDs are, whether they are working, when supplies expire, who receives alerts, who is trained, and how your team responds when every second matters.
The old model was simple: install the AED and hope it works.
The better model is more active: monitor it, maintain it, connect it where appropriate, train people to use it, and make it part of a real emergency plan.
A Practical Reminder for Employers
Technology can help you track the AED. Training helps your people use it. The strongest safety plans do both.
At In-Pulse CPR, we believe workplace safety should be practical and hands-on. Technology can help organizations manage AEDs more reliably, especially across multiple locations, but the people on site still need to know what to do.
An AED on the wall is a good start.
An AED that is ready, maintained, easy to find, and supported by trained employees is much better.
That is the real promise of IoT and AI-driven AED management. Not replacing people. Not turning emergency response into a software project. Just making sure the silent safety device on the wall is actually ready when someone’s life depends on it.
Need CPR and AED Training for Your Team?
In-Pulse CPR provides hands-on American Heart Association CPR, AED, First Aid, and BLS training for workplaces, schools, healthcare teams, and community organizations.
Request Onsite Training
It all starts with a well-trained team. Connected AEDs, smart cabinets, and readiness alerts can help, but they do not replace people who know how to respond. In a real emergency, someone has to recognize cardiac arrest, call 911, begin CPR, bring the AED, and follow the device prompts with confidence. That confidence comes from hands-on practice, not guesswork. In-Pulse CPR provides American Heart Association CPR and AED training in
, helping workplaces build safer, better-prepared teams before an emergency happens.
 by Benjamin Roussey
by Benjamin Roussey