An Innocent Child

 by Melanie Pinette
by Melanie Pinette- Apr 23, 2026
- 0
- Category: CPR in Pennsylvania, Why do we need CPR training?
Written by Melanie Pinette, Updated 2026 by Val
Love is one of the most powerful human emotions—especially the kind shared between a parent and child. Ask any mom or dad what they love most about being a parent, and you’ll see it instantly: a warm smile, followed by a list that could stretch a mile long.
Of course, there are also those unforgettable moments… like a quick trip to the store that turns into a full-blown meltdown because a ring-pop before nap time somehow feels like a perfectly reasonable request. Through every high and low, one truth remains steady:
“We wouldn’t trade them for the world.”
Every parent dreams about the future. The strong, hardworking man their son will become. The confident, accomplished woman their daughter will grow into. We do everything we can to guide them, teach them right from wrong, and protect them from a world that doesn’t always play fair.
Growing up looked different for many of us. Riding in the back of pickup trucks. No helmets. Streetlights were the only curfew we needed. Today, we wrap our kids in layers of protection—helmets, pads, supervision, safeguards. And that’s a good thing.
But when it comes to one of the most important forms of protection… many parents fall short.
When people think of CPR, they picture scenes from movies.
“It’ll never happen to me.”
“I’ve seen it on TV—I could figure it out.”
But real life doesn’t follow a script.
Life is fragile. It can change in an instant.
In 1995, I lost my son to SIDS (Sudden Infant Death Syndrome). There are no words strong enough to describe that kind of loss. As the saying goes, a parent should never have to bury their child. It’s a pain that reaches beyond anything physical—it settles deep and stays.
Some people never recover from that kind of grief. Others try to transform it into something meaningful.
For me, that moment came while watching the medics and firefighters work tirelessly to save my baby. Their determination, their skill, their refusal to give up—it left a permanent mark on me.
Years later, after a great deal of reflection, I made a decision: I went back to school and became an EMT.
Not long after, I found In-Pulse CPR. They were looking for instructors and assistants. It felt like everything had aligned—an opportunity to take something tragic and turn it into something that could help others.
I met Troy Bowman… and was hired on the spot.
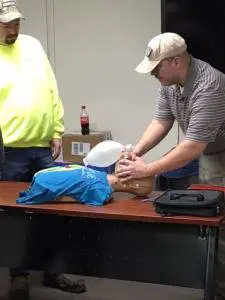
Today, I help teach others a skill that I wish every parent truly understood.
A Simple Question Every Parent Should Answer
One of the first questions I ask new parents is:
“Are you certified in infant CPR?”
The most common response?
“I’m not certified, but I’m sure I could do it if I had to.”
That answer is more common than you’d think—and more dangerous than most realize.
CPR isn’t complicated, but it is specific.
And those specifics matter.
What Many Parents Don’t Realize
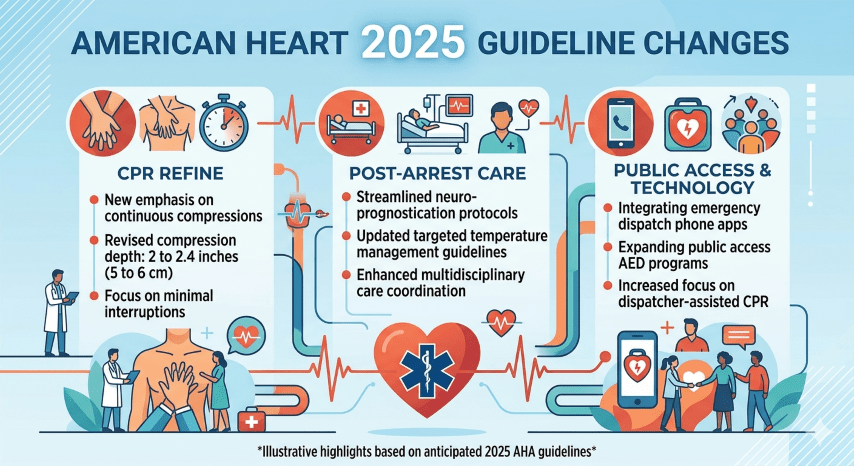
- Infant CPR is different from child and adult CPR
- Proper hand placement and compression depth are critical
- Timing, rhythm, and airway techniques must be learned—not guessed
- In an emergency, there is no time to “figure it out”
- Confidence comes from hands-on practice, not observation
In-Pulse CPR is built around one simple goal: helping people feel prepared when it matters most. Our team is dedicated to making sure you don’t just memorize steps—you understand what you’re doing and why it works.
Take a moment to look at upcoming classes.
It’s a small investment of time… but one that could mean everything.
Because when it comes to the people we love most,
“good enough” should never be the plan.