CPR Chest Compression Technique: How to Push Hard, Push Fast, and Help Save a Life
Estimated reading time: 12 minutes
Sudden cardiac arrest does not usually give people much time to think.
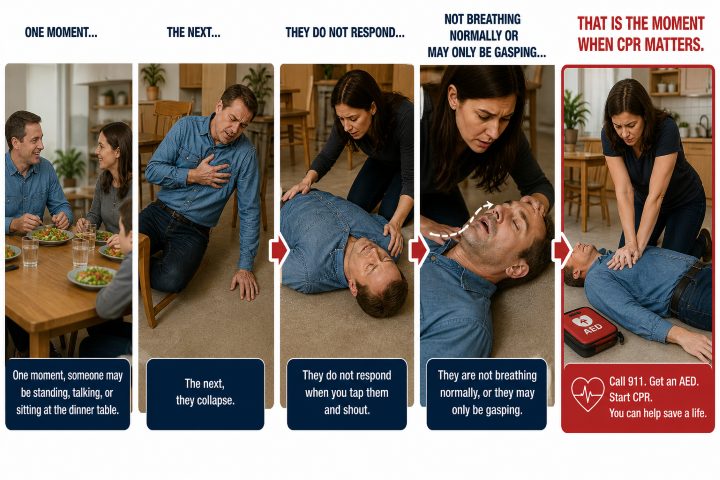
The tragedy that just happens…
One moment, someone may be standing, talking, or sitting at the dinner table. The next, they collapse. They do not respond when you tap them and shout. They are not breathing normally, or they may only be gasping.
That is the moment when CPR matters.
Chest compressions are one of the most important parts of CPR because they help move blood through the body when the heart is no longer pumping effectively. They help send blood to the brain, heart, and other vital organs until emergency medical services arrive or an AED can be used.
The technique is simple, but it needs to be done well. Good CPR is not gentle. It is not slow. It is not something you do for a few seconds and then stop to see if it worked. High-quality CPR means pushing hard enough, fast enough, allowing the chest to come back up, and keeping pauses as short as possible.
What Chest Compressions Actually Do
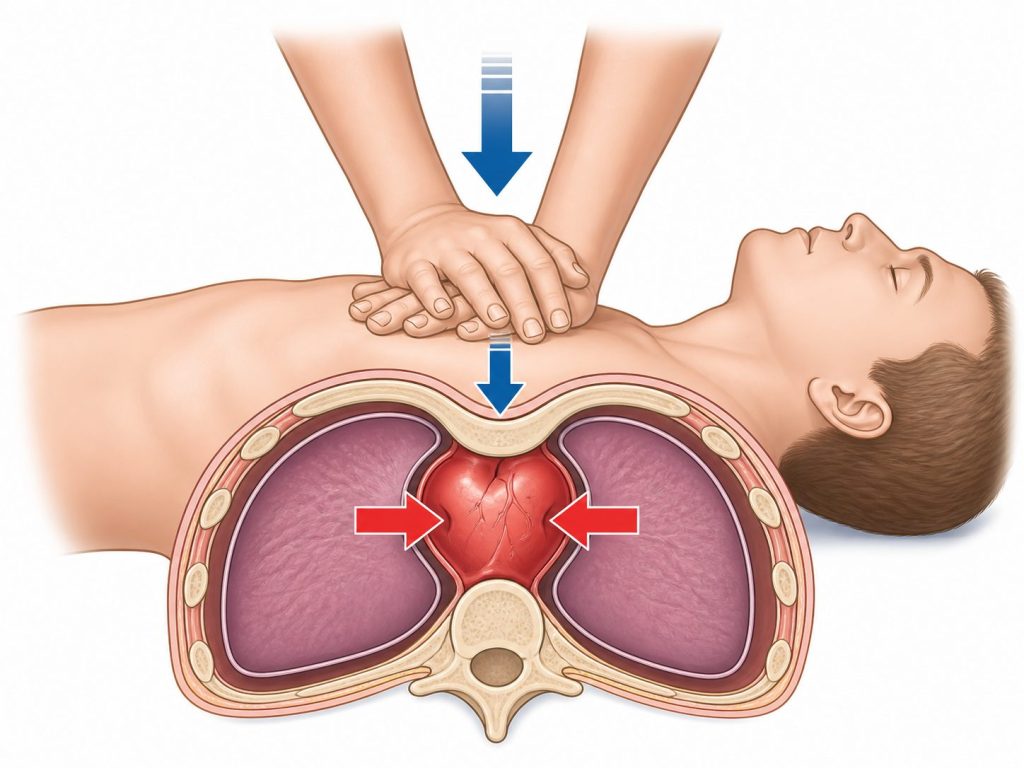
When someone is in cardiac arrest, the heart has stopped pumping blood the way it should. Without blood flow, the brain and organs quickly begin to suffer from lack of oxygen.
Chest compressions act like a temporary pump.
Each time you press down on the chest, you help squeeze the heart and move blood forward. Each time you release, the chest rises back up and the heart can refill. Then you press again.
It is not perfect. CPR does not work exactly like a normal heartbeat. But it can buy precious time. In a cardiac arrest emergency, that time matters.
The American Heart Association identifies several pieces of high-quality CPR, including a compression rate of 100 to 120 compressions per minute, adult compression depth of at least 2 inches, full chest recoil, and limited interruptions.
First, Make Sure CPR Is Needed
Before starting chest compressions, check the person.
Tap their shoulder and shout something direct, such as, “Are you okay?”
If they do not respond and they are not breathing normally, call 911 or tell someone nearby to call. If an AED is available, send someone to get it right away.
Do not let gasping fool you. A person in cardiac arrest may make strange, irregular gasping sounds. That is not normal breathing. If the person is unresponsive and not breathing normally, start CPR.
Proper Hand Placement for Adult CPR
For adult CPR, place the person flat on their back on a firm surface. Kneel beside them.
Place the heel of one hand in the center of the chest. Your hand should be on the lower half of the breastbone, not down on the stomach and not off to the side on the ribs. Place your other hand on top. Interlace your fingers or keep them lifted so the pressure stays on the heel of your hand.
Your hands should be centered. This matters because poor hand placement can make compressions less effective and may increase the chance of injury.
The Red Cross describes adult CPR hand position as two hands centered on the chest, with shoulders directly over the hands and elbows locked.
“Liability fades when skills ascend. CPR training: the smartest hedge against disaster.”
Troy Bowman
Use Your Body Weight, Not Just Your Arms
This is one of the biggest technique details people miss.
CPR is not supposed to be an arm workout.
If you bend your elbows and try to push with your arms, you will get tired quickly. Your compressions may also become too shallow.
Instead, get your shoulders directly above your hands. Lock your elbows. Keep your arms straight. Use your upper body weight to press straight down into the chest.
You should be moving from your torso, not pumping from your elbows.
A good way to picture it: your shoulders, arms, and hands should stack over the center of the chest. That straight line helps you push deeper and stay more consistent.
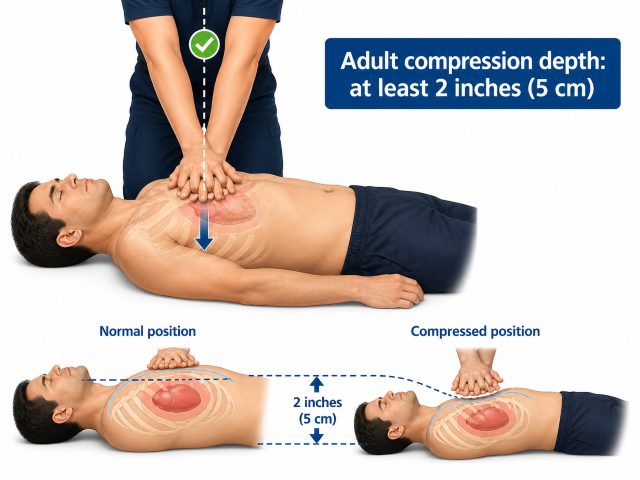
How Deep Should Chest Compressions Be?
For adults, chest compressions should be at least 2 inches deep.
That is deeper than many people expect.
In a real emergency, shallow compressions are a common problem. People are often afraid to push hard. They worry about hurting the person. That reaction is understandable, but cardiac arrest is already life-threatening. The person needs blood flow.
You may feel or hear cracking during CPR. This can happen. Do not stop just because of that. Keep going unless the person starts breathing normally, an AED tells you to pause, EMS takes over, the scene becomes unsafe, or you physically cannot continue.
Gentle pressing is not enough. Effective compressions require real force.
How Fast Should Chest Compressions Be?
The recommended compression rate is 100 to 120 compressions per minute.
Too slow, and you may not move enough blood. Too fast, and the compressions may become shallow or the chest may not fully return to its normal position between pushes.
People often use familiar songs to remember the rhythm, but the rhythm is only part of the skill. You still need the right depth, hand placement, and recoil.
Push hard. Push fast. Stay steady.
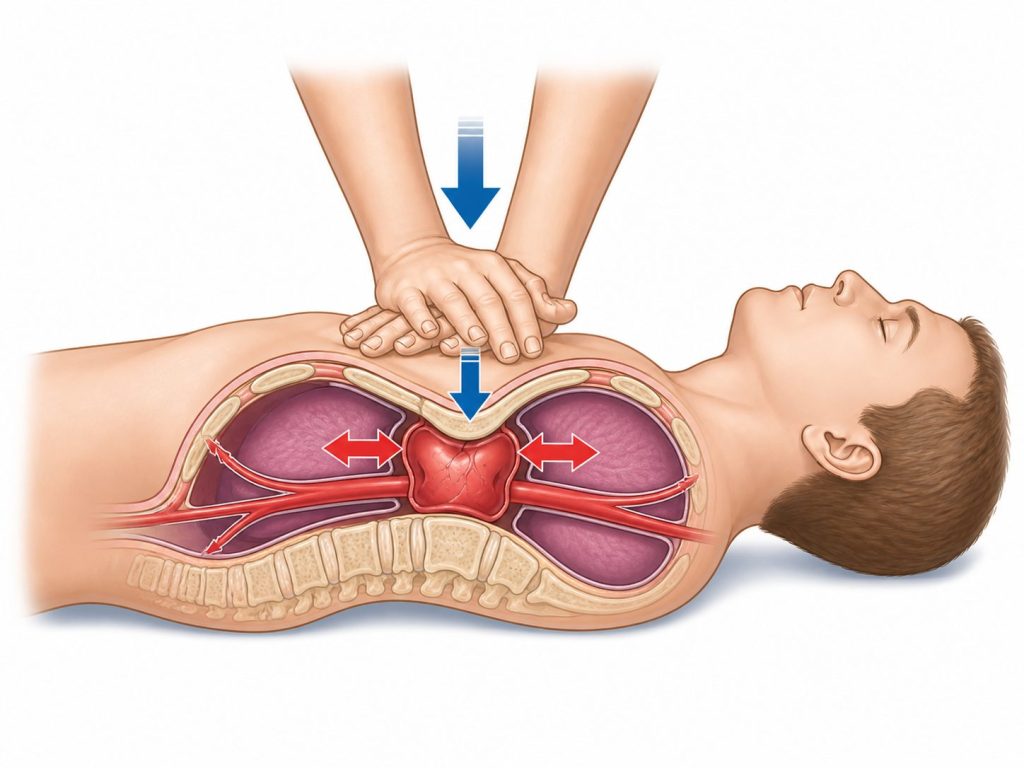
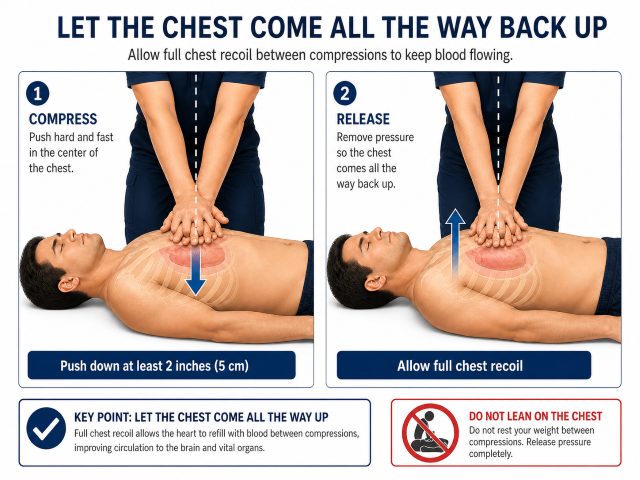
Let the Chest Come All the Way Back Up
Chest recoil is the release after each compression.
This part is easy to overlook. Some people push down correctly but keep leaning on the chest between compressions. That can reduce how well the heart refills with blood before the next push.
After every compression, let the chest return to its normal position. Do not lift your hands off the chest, but do release your weight.
CPR is not just push, push, push. It is push and release. Push and release. The release matters.
The American Heart includes allowing the chest to return to normal position after each compression as one of the key CPR points.
Do Not Stop Unless You Have To
Every pause in chest compressions reduces blood flow.
That does not mean you never pause. You may need to pause when an AED tells you to stop touching the person. You may need to switch with another rescuer. EMS may take over. The person may begin breathing normally.
But avoid unnecessary stops.
Do not stop every few seconds to check for a pulse. Do not stop because you are unsure if you are doing it perfectly. Do not stop because it feels awkward.
If another trained person is with you, switch compressors about every two minutes if possible. CPR is tiring, and compression quality can drop as the rescuer gets fatigued. The American Heart Association notes that compression depth can begin to decrease after 90 to 120 seconds of CPR.
Hands-Only CPR vs. CPR With Breaths
For many adult sudden cardiac arrest emergencies, hands-only CPR can help by keeping blood moving until more advanced help arrives. This is especially important for bystanders who are not trained or who are unsure about giving breaths.
Hands-only CPR means calling 911, sending for an AED, and giving continuous chest compressions.
Trained rescuers may provide rescue breaths along with compressions, depending on the situation and their level of training. Breaths are especially important in many child and infant emergencies, drowning incidents, and breathing-related emergencies.
This is one reason CPR training matters. Adults, children, and infants are not handled exactly the same way.
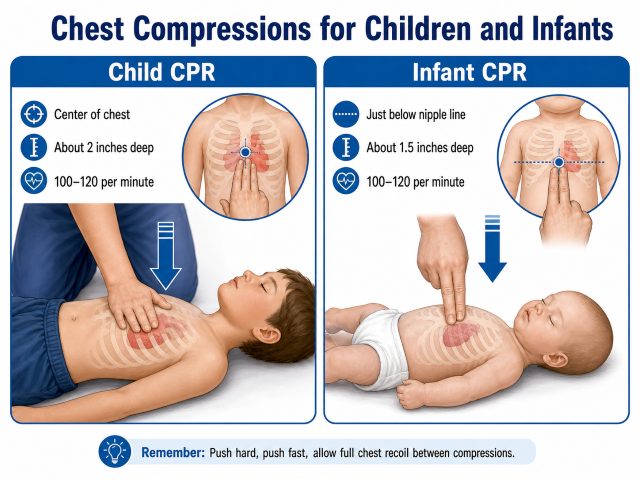
Chest Compressions for Children and Infants
The basic idea is the same: push hard, push fast, and allow the chest to come back up.
But the technique changes based on the size and age of the person.
For a child, you may use one hand or two hands, depending on the child’s size. The compression depth is about 2 inches, with a rate of 100 to 120 compressions per minute. For an infant, compressions are shallower, about 1.5 inches, and may be done with two fingers or with the two-thumb encircling technique when properly trained.
The most important point for parents, teachers, childcare workers, coaches, and healthcare staff is this: child and infant CPR should be practiced hands-on. Reading the steps helps, but practice builds confidence.
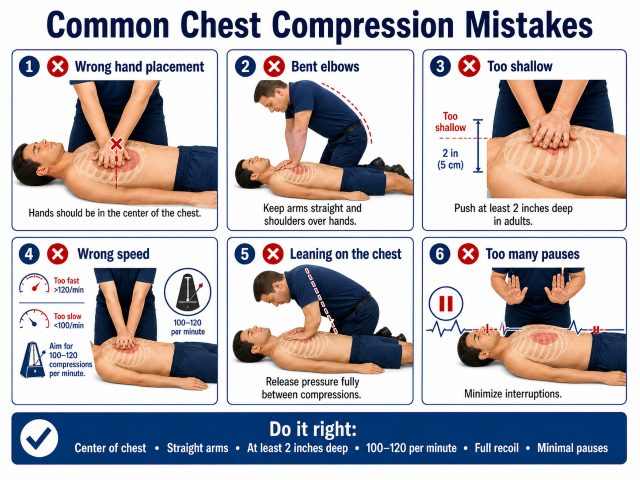
Common Chest Compression Mistakes
Most CPR mistakes are fixable with practice.
Some of the most common include placing the hands too low, bending the elbows, rocking back and forth instead of pushing straight down, not pressing deep enough, pressing too fast, leaning on the chest between compressions, and stopping too often.
Another common mistake is waiting too long to begin.
People freeze because they are afraid of doing something wrong. But in cardiac arrest, doing nothing is usually the worst option. Call 911, get an AED if one is nearby, and start compressions.
Why Hands-On CPR Practice Matters
You can read about CPR in a few minutes. Learning how it feels takes practice.
In a hands-on CPR class, students learn where to place their hands, how deep to press, how fast to go, and how to avoid leaning on the chest. Instructors can correct small technique problems before they become real emergency problems.
Many people are surprised by how firm chest compressions need to be. Others realize they were bending their elbows or pressing in the wrong spot. Practice makes those details more natural.
That matters because emergencies do not wait for people to feel ready.
When Should You Stop CPR?
Keep giving CPR until one of these things happens:
EMS arrives and takes over. An AED tells you to pause. The person starts breathing normally. The scene becomes unsafe. You are too exhausted to continue.
Until then, keep going.
Key Takeaways
CPR chest compressions are crucial for maintaining blood flow during cardiac arrest, so act quickly when someone collapses.
Push hard and fast: compress at least 2 inches deep and at a rate of 100 to 120 compressions per minute.
Ensure proper hand placement by placing the heel of one hand on the lower half of the breastbone, with the other hand on top.
Allow the chest to fully recoil between compressions for effective blood flow and avoid unnecessary pauses during CPR.
Practice hands-on techniques in CPR classes to build confidence and improve your skills for real emergencies.
Final Thought
CPR chest compressions are simple, but they are powerful.
Put your hands in the center of the chest. Lock your elbows. Keep your shoulders over your hands. Push at least 2 inches deep for an adult. Keep a steady rate of 100 to 120 compressions per minute. Let the chest rise fully between compressions. Keep pauses short.
You do not need to be perfect to make a difference. But good technique helps.
When someone collapses from sudden cardiac arrest, the best CPR is the CPR that starts. Call 911, send for an AED, and begin chest compressions. Push hard. Push fast. Keep going until help arrives.
In-Pulse CPR offers hands-on American Heart Association CPR, AED, First Aid, and BLS certification classes for new and renewing students. Our classes give you the chance to practice these skills, ask questions, and leave knowing what to do when an emergency happens.
No. Rib or cartilage injuries can happen during CPR, especially on adults. If the person is in cardiac arrest, blood flow is the priority. Keep going unless the person starts breathing normally, an AED tells you to pause, EMS takes over, the scene becomes unsafe, or you are physically unable to continue.
Is hands-only CPR enough?
Hands-only CPR can help in many adult sudden cardiac arrest emergencies, especially when the rescuer is not trained or is unsure about giving breaths. Call 911, send someone for an AED, and give continuous chest compressions. Trained rescuers should follow their training, which may include rescue breaths.
What is the most common CPR compression mistake?
One of the most common mistakes is not pushing deep enough. Other common mistakes include bending the elbows, placing the hands too low, leaning on the chest, pushing too fast or too slow, and stopping too often.
Why should I take a CPR class if I can read the steps online?
Reading the steps helps, but CPR is a physical skill. In a hands-on class, you can practice the correct hand placement, compression depth, rate, and chest recoil. You also get feedback from an instructor, which makes a big difference in confidence and technique. It adds value to add to a resume’ and builds confidence so you don’t panic when an emergency happens.
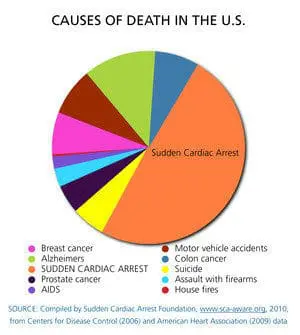
Here is something worth knowing. Sudden cardiac arrest is still one of the leading causes of death in the United States. More than 350,000 cardiac arrests happen outside of hospitals each year. That is close to 1,000 people every day.
The survival rate is still far too low. About 9 out of 10 people who suffer cardiac arrest outside the hospital do not survive.
But those first few minutes can change everything.
When someone nearby starts CPR right away, it can double or even triple the person’s chance of survival. When an AED is used quickly, the odds can improve even more.
That is why CPR training matters. Cardiac arrest does not usually happen in a hospital with a medical team standing nearby. It often happens at home, at work, at church, in a gym, on a ball field, or in a grocery store.
In that moment, the person who helps first is usually an ordinary person standing close by.
Everyone should learn CPR. You hope you never need it, but if you do, there is no substitute for knowing what to do.
Sudden cardiac arrest does not always come with a warning. A person may be talking, laughing, working, or eating dinner, and then suddenly collapse. Not planned, and never convenient.
They may not respond when you tap their shoulder and shout. They may not be breathing normally. Sometimes they may only gasp, which can be confusing because it looks like breathing, but it is not normal breathing.
That is the moment when quick action matters.
Many cardiac arrests outside the hospital happen at home. That means the person who needs help may be someone you know: a spouse, parent, grandparent, friend, coworker, or neighbor. The first few minutes are critical. Starting CPR right away can help keep blood moving to the brain and vital organs until emergency responders arrive.
What is sudden cardiac arrest?
Sudden cardiac arrest happens when the heart suddenly stops pumping blood the way it should. In many cases, it is caused by a problem with the heart’s electrical system. Instead of beating normally, the heart may quiver or fall into a dangerous rhythm. Blood stops moving through the body, and the person quickly becomes unconscious.
Cardiac arrest is not the same as a heart attack.
A heart attack is usually a circulation problem. Blood flow to part of the heart muscle is blocked. The person may still be awake and may complain of chest pressure, shortness of breath, sweating, nausea, or pain in the arm, jaw, back, or stomach.
Cardiac arrest is different. The person is usually unresponsive and not breathing normally. They need CPR right away, and an AED if one is nearby.
Signs someone may need CPR
Start CPR if the person:
Suddenly collapses
Does not respond when you tap and shout
Is not breathing normally
Is only gasping
Gasping can happen during cardiac arrest. Do not wait around hoping it turns into normal breathing. If the person is unresponsive and not breathing normally, start CPR.
Hands-Only CPR steps for adults
Call 911 immediately. Put the phone on speaker if you can. This lets you talk with the dispatcher while keeping your hands free.
Send someone for an AED. If other people are nearby, be direct. Point to one person and say, “You, get the AED.” A clear instruction works better than a general shout into the room.
Start chest compressions. Place the heel of one hand in the center of the chest. Put your other hand on top. Keep your arms straight and your shoulders over your hands.
Push hard and fast. Press down at least 2 inches on an adult chest, but not more than 2.4 inches. Let the chest come all the way back up between compressions. Aim for 100 to 120 compressions per minute.
Keep going. Do not stop unless emergency responders take over, the person starts breathing normally, an AED is ready to analyze, or you are too tired to continue.
You do not have to do it perfectly. The biggest mistake is doing nothing.
How an AED helps
An AED, or automated external defibrillator, is a device that can check the heart’s rhythm and deliver a shock if one is needed. AEDs are designed for regular people to use, not just medical professionals.
Today, many workplaces, gyms, schools, airports, churches, and public buildings have AEDs nearby. If one is available, use it.
Turn the AED on and follow the voice prompts. The device will tell you what to do step by step. Place the pads on the person’s bare chest as shown in the pictures on the pads. Make sure no one is touching the person while the AED checks the heart rhythm.
If the AED tells you to give a shock, make sure everyone is clear, then press the shock button if instructed. After the shock, or if no shock is advised, start CPR again right away and keep following the AED prompts.
The AED will guide you. Listen to it, stay calm, and keep helping.
When rescue breaths may be needed
Hands-Only CPR is recommended for many adult sudden-collapse emergencies, especially when the person is unresponsive and not breathing normally.
There are times when conventional CPR with rescue breaths may be especially important, including:
Drowning
Drug overdose
Children and infants
Breathing-related emergencies
Situations where the collapse may have been caused by lack of oxygen
This is one reason CPR training is so valuable. A good class gives you practice with chest compressions, rescue breaths, AED use, choking care, and different age groups.
Who is at higher risk?
Sudden cardiac arrest can happen to anyone, but some people have a higher risk. This may include people with:
A previous heart attack
Known heart disease
High blood pressure
Diabetes
High cholesterol
Smoking history
Obesity
Certain inherited heart rhythm conditions
Still, cardiac arrest can happen without obvious warning signs, even to people who seem healthy. That is why CPR and AED training should not be limited to healthcare workers.
Why CPR training matters
In a real emergency, it is normal to freeze for a second. Most people do. The room feels loud and quiet at the same time. Everyone looks around, hoping someone else knows what to do.
Training helps you get past that moment.
You know where to place your hands. You know how hard to push. You know how to use an AED. You know what to do until help arrives.
You may never need to use CPR. But if you do, those few minutes could make all the difference. CPR gives a person a chance they may not have had otherwise.
I was recently forwarded another internet article referring to “cough CPR” and asked if this is something we should be considering.
This topic has been around for years. It shows up in emails, social media posts, and online articles. The message usually says that if you are alone and think you are having a heart attack, you should cough hard and repeatedly until help arrives.
It sounds helpful. It sounds simple. But it can also be misleading.
At In-Pulse CPR, we do not endorse “cough CPR,” and we do not teach it in our CPR classes.
What Is “Cough CPR”?
Cough CPR is usually described as a method of repeated, forceful coughing that a person can do if they think they are having a heart problem while alone.
The idea is that coughing may briefly increase pressure in the chest and help move blood during certain abnormal heart rhythms.
There are a few very specific medical situations where a physician or nurse may instruct a patient to cough. But that is not the same as CPR, and it is not something the general public should rely on during a medical emergency.
Why Isn’t “Cough CPR” Appropriate in CPR Training Courses?
I do not feel that “cough CPR” should be taught to lay rescuers.
It complicates the basic teachings of CPR and may confuse people about what CPR is actually for.
The finding that signals the need for CPR is that the victim is unresponsive and not breathing normally. An unresponsive person will not be able to perform “cough CPR.”
That alone should tell us this does not belong in a basic CPR class.
There have been situations where a cough technique has been used under a physician’s direction. These are specific medical situations and always involve direct medical supervision. The patient is usually being monitored, and medical staff are right there.
Used for the wrong reason, or in the wrong way, it could be dangerous. More importantly, it could delay someone from doing what they really need to do: call 911 and get emergency medical help.
My Recommendation
If you think you may be having a heart attack, the first step is not to cough.
The first step is to call 911 immediately.
Do not wait to see if it passes. Do not try to drive yourself unless there is truly no other option. If you are alone, call 911 and put the phone on speaker so the dispatcher can talk with you.
If you are driving, pull safely to the side of the road and call 911. If you cannot call, try to get someone’s attention and get help.
Aspirin may be recommended in some suspected heart attack situations, but it is not right for everyone. Current guidance is to call 911 first and follow the dispatcher’s or medical provider’s instructions. Do not delay emergency care to take aspirin.
If someone else collapses, is unresponsive, and is not breathing normally, call 911, start CPR, and get an AED if one is available.
That is the CPR message we want people to remember.
Are There Any Situations When “Cough CPR” Is Appropriate?
There are times when coughing may be helpful, but those situations are very limited.
One example is during cardiac catheterization. During this procedure, a patient may develop a sudden abnormal heart rhythm. Because the patient is being continuously monitored, the medical team may see the rhythm problem right away. Before the patient loses consciousness, a physician or nurse may instruct the person to cough repeatedly.
This may help maintain blood flow for a short time and may help keep the person conscious until the rhythm is treated or stops on its own.
But again, this is happening in a medical setting. The patient is on a monitor. A physician or nurse is present. Emergency treatment is available immediately.
That is very different from being alone at home, at work, or in a car after reading advice online.
Bottom Line
“Cough CPR” should be limited to specific monitored medical situations where a healthcare professional gives that instruction.
It should not be taught as a public CPR skill.
For the general public, the recommendation remains simple:
Call 911. Start CPR if the person is unresponsive and not breathing normally. Use an AED as soon as possible. Follow the dispatcher’s instructions.
At In-Pulse CPR, we will continue to teach the skills that people are most likely to need in a real emergency. Simple steps. Hands-on practice. Clear action.
That is what saves lives.
Author: Mollie Bowman, Owner and Primary Instructor for In-Pulse CPR Updated: 2026
The Silent Sentinel: The Rise of IoT and AI-Driven AED Management in 2026
For years, an AED was treated like a quiet safety box on the wall.
A business bought it, mounted it in a hallway, placed a sign above it, and maybe added it to a monthly inspection checklist. After that, everyone hoped it would be ready if the worst happened.
You could call it the “install and hope” approach.
You installed the AED. You hoped the battery was good. You hoped the pads had not expired. You hoped nobody moved it, blocked it, or forgot to check the status light.
That approach may have been common, but it was never ideal. In 2026, it is becoming even harder to justify.
AED management is changing. New connected AED systems, smart cabinets, cloud-based monitoring, emergency registries, and AI-supported feedback are turning AEDs from passive equipment into active parts of a workplace safety plan.
That does not mean every AED is suddenly a robot doctor on the wall. It means businesses now have better tools to answer a basic but important question:
Is our AED actually ready?
The Problem with the Old AED Model
Most AED problems are not dramatic. They are ordinary.
A battery gets weak. Pads expire. A cabinet gets blocked by storage boxes. The AED is moved during remodeling and never returned to its original spot. The person responsible for checking it changes jobs, and the task quietly disappears.
Nobody notices until the emergency happens.
That is the risk with old-school AED management. It depends heavily on people remembering to inspect a device that may sit unused for years, but still has to work perfectly the moment someone collapses.
In a cardiac emergency, those small maintenance details are no longer small. CPR needs to begin quickly. The AED needs to be found quickly. The device needs to turn on, guide the rescuer, analyze the heart rhythm, and deliver a shock if needed.
“I thought someone checked it” is not much of a safety plan.
Connected AEDs Make Readiness Easier to Track
IoT stands for Internet of Things. In plain English, it means everyday equipment can connect and send information.
For AEDs, that is a big deal.
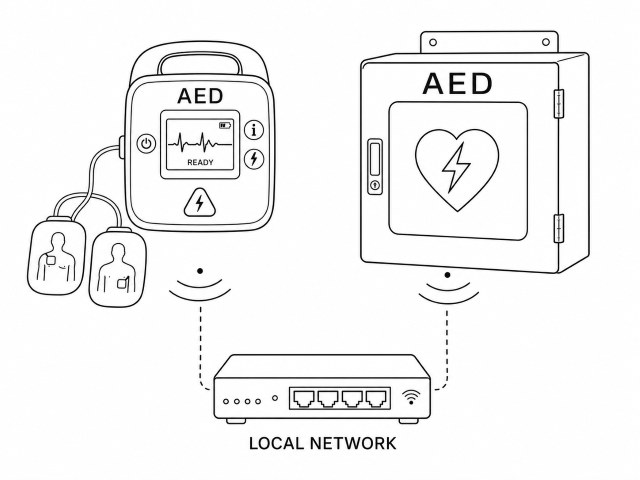
A connected AED or smart AED cabinet may be able to report whether the device is ready, whether the battery needs attention, whether the pads are nearing expiration, or whether the cabinet has been opened.
Instead of relying only on a clipboard hanging nearby, the system can send alerts when something needs to be fixed.
For a small office with one AED, that might prevent a missed battery replacement. For a company with several locations, it can make a much bigger difference.
A safety manager can see which AEDs are ready and which ones need attention without calling every building, school, branch, warehouse, or clinic. That kind of visibility matters, especially when one missed inspection can leave a device unavailable at the worst possible time.
The real benefit is simple: AED readiness becomes something you can verify instead of something you assume.
The 2026 Readiness Audit
If your organization has an AED, these are the kinds of questions worth asking before an emergency happens:
Do we have a digital log or written record of our recent AED checks?
Do we know when the pads and battery expire?
Is our AED registered with local dispatch, PulsePoint, or another AED registry if available in our area?
Who receives an alert if our AED cabinet is opened right now?
Is the AED easy to find, or is it blocked by furniture, boxes, or locked doors?
Do employees know who calls 911, who starts CPR, and who brings the AED?
Smart Cabinets Add Another Layer of Protection
The cabinet matters too.
An AED mounted inside a clean, climate-controlled office hallway has a different environment than one placed near a warehouse entrance, school gym, church lobby, manufacturing floor, outdoor recreation area, or busy public building.
Heat, cold, dust, humidity, and foot traffic can all create problems over time.
Some newer AED cabinets can monitor conditions around the device. Depending on the system, they may track temperature, humidity, cabinet access, or whether the AED has been removed.
That may sound like a small upgrade, but it solves a real problem. AED pads and batteries are not meant to be forgotten forever. A device can look fine from the outside while still needing attention inside the case.
Smart cabinets help catch those issues before an emergency exposes them.
AI Can Help During the Emergency
Connected technology can help before the emergency. Artificial intelligence and improved AED feedback can help during the emergency.
This is where the technology gets more interesting, but it should still be explained in practical terms.
Some newer AEDs and CPR feedback systems can help guide rescuers on compression depth and rate. If the person doing CPR is pressing too shallow, moving too fast, or slowing down, the device may give voice prompts to help improve CPR quality.
That matters because CPR is physically demanding. In a real emergency, people are scared, adrenaline is high, and even trained responders can lose rhythm or pause too long.
AI-supported feedback does not replace CPR training. It gives the rescuer support in the moment.
The best way to think of it is this: training prepares the person, and the device helps coach them while they work.
Reducing Pauses in CPR Matters
One of the major goals in cardiac arrest response is reducing unnecessary pauses in chest compressions.
Every time compressions stop, blood flow drops. That is why modern CPR training places so much emphasis on keeping compressions going, switching rescuers when needed, and resuming CPR immediately after a shock is delivered.
AED technology continues to improve in this area too. Some systems are designed to reduce interruptions during rhythm analysis and help rescuers stay focused on high-quality CPR.
For employers, the takeaway is not that the AED does everything on its own. It does not.
Someone still has to recognize the emergency, call 911, start compressions, bring the AED, expose the chest, apply the pads, and follow the prompts.
Technology can make the process smoother. Trained people still make the response happen.
AEDs Are Becoming Part of the Larger Emergency Network
One of the biggest changes in AED management is that these devices are becoming more connected to the wider emergency response system.
In the past, a workplace AED often existed only for that building. It might be available to employees, customers, students, patients, or visitors inside the facility, but local emergency responders may not have known it was there.
That is starting to change.
AED registries and emergency response apps can help identify where AEDs are located. In some areas, this can help dispatchers, first responders, or trained community members find the nearest available AED faster.
This matters because cardiac arrest does not politely happen next to the best-prepared person in the building.
It may happen in a parking lot, on a sidewalk, at a youth sports event, in a church fellowship hall, outside a school, or near a neighboring business. If an AED is nearby and ready, it may be useful beyond the four walls of the organization that purchased it.
That is a major shift. A workplace AED is no longer just a private safety item. It can become part of the community’s emergency response network.
Better Data Can Help After the AED Is Used
AED management does not end when the device is opened.
Modern AEDs can collect important event information, such as when the device was turned on, whether a shock was advised, when shocks were delivered, and how the response unfolded.
That information can be useful for EMS documentation, hospital care, internal review, and future training. It can also help leaders understand what went well and what needs improvement.
After a real emergency, people often have questions.
Did we start CPR quickly enough?
Did someone call 911 right away?
Was the AED easy to find?
Did employees know what to do?
Were there delays we could prevent next time?
Event data can help answer those questions more clearly.
It can also help support the people who responded. Performing CPR or using an AED in a real emergency is not a small thing. Employees may replay the event in their heads afterward, wondering if they did enough.
A thoughtful post-event review can help them understand what happened, what actions they took, and how their response helped.
Cybersecurity Should Be Part of the Conversation
Any time medical equipment connects to a network, IT departments are going to ask questions. They should.
Connected AED systems may raise concerns about Wi-Fi access, data security, software updates, privacy, and who receives device alerts.
Those are fair questions, especially for schools, healthcare offices, government buildings, large employers, and companies with strict technology policies.
Before choosing a connected AED system, it is worth asking:
How does the device connect?
Does it use Wi-Fi, cellular service, or another method?
What information is being sent?
Who receives alerts?
Is the data encrypted?
What happens if the connection goes down?
How are updates handled?
Does the system require access to the company’s internal network?
The point is not to make AED ownership more complicated. It is to make sure the system improves safety without creating unnecessary headaches for IT, compliance, or operations.
A connected AED should make readiness easier to manage, not harder.
The Human Side Still Comes First
Even with smart cabinets, cloud dashboards, AED registries, AI feedback, and better data sharing, the most important part of the response is still human.
Someone has to notice the emergency.
Someone has to call 911.
Someone has to start CPR.
Someone has to bring the AED.
Someone has to keep going until EMS arrives.
That is why AED technology and CPR training belong together.
A connected AED can alert you when pads expire. It cannot build confidence in your staff by itself.
AI feedback can coach compressions. It cannot replace hands-on practice.
A registry can show where the AED is located. It cannot guarantee someone will know what to do under pressure.
The strongest safety programs combine reliable equipment with trained people.
That means employees know where the AED is. They know who calls 911. They know how to start compressions. They have practiced with a training AED. They understand that the device will talk them through the steps, but they still need to act.
That confidence usually does not come from reading a policy. It comes from practice.
Moving Beyond “Install and Hope”
In 2026, AED management should not be treated as a one-time purchase.
Buying the AED is the start. Mounting it in a visible place is important. But the real goal is readiness.
That means knowing where your AEDs are, whether they are working, when supplies expire, who receives alerts, who is trained, and how your team responds when every second matters.
The old model was simple: install the AED and hope it works.
The better model is more active: monitor it, maintain it, connect it where appropriate, train people to use it, and make it part of a real emergency plan.
A Practical Reminder for Employers
Technology can help you track the AED. Training helps your people use it. The strongest safety plans do both.
At In-Pulse CPR, we believe workplace safety should be practical and hands-on. Technology can help organizations manage AEDs more reliably, especially across multiple locations, but the people on site still need to know what to do.
An AED on the wall is a good start.
An AED that is ready, maintained, easy to find, and supported by trained employees is much better.
That is the real promise of IoT and AI-driven AED management. Not replacing people. Not turning emergency response into a software project. Just making sure the silent safety device on the wall is actually ready when someone’s life depends on it.
Need CPR and AED Training for Your Team?
In-Pulse CPR provides hands-on American Heart Association CPR, AED, First Aid, and BLS training for workplaces, schools, healthcare teams, and community organizations.
It all starts with a well-trained team. Connected AEDs, smart cabinets, and readiness alerts can help, but they do not replace people who know how to respond. In a real emergency, someone has to recognize cardiac arrest, call 911, begin CPR, bring the AED, and follow the device prompts with confidence. That confidence comes from hands-on practice, not guesswork. In-Pulse CPR provides American Heart Association CPR and AED training in Minnesota, Florida, Pennsylvania, and Tennessee, helping workplaces build safer, better-prepared teams before an emergency happens.
Cardiac arrest is still one of the leading causes of death in the United States. It can happen suddenly, often when an electrical problem in the heart causes it to stop pumping blood the way it should.
When that happens, every minute counts.
The person does not need a perfect rescuer. They need someone nearby to notice something is wrong, call 911, start CPR, and get an AED if one is available. That first response, even from a regular bystander, can make a real difference before EMS arrives.
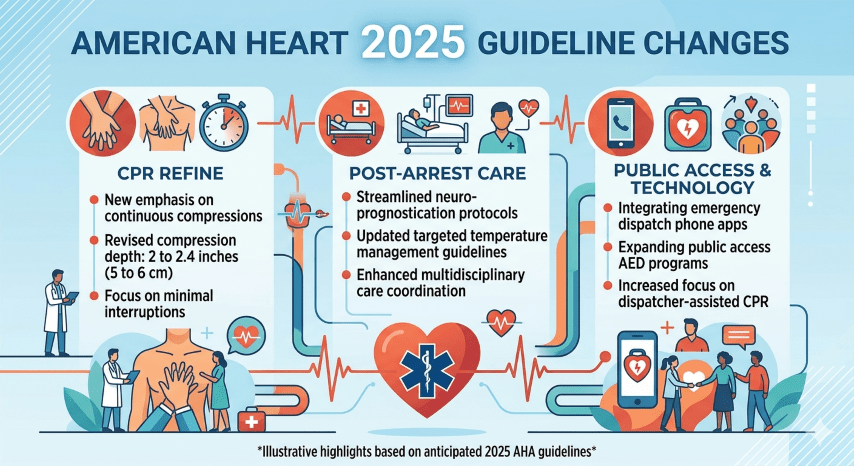
The 2025 American Heart Association Guidelines for CPR and Emergency Cardiovascular Care continue to stress that lifesaving care is not just one person’s job. Bystanders, 911 dispatchers, coworkers, teachers, coaches, healthcare workers, EMS crews, and hospitals all play a part.
The big message is simple: act quickly, work together, and keep CPR skills fresh.
Quick Action Still Matters Most
If someone collapses and is not breathing normally, call 911 right away. Put the phone on speaker so the dispatcher can help guide you.
For people who are not trained in CPR, the American Heart Association still supports Hands-Only CPR. Push hard and fast in the center of the chest until help arrives or an AED is ready to use.
For people who are trained in CPR, rescue breaths may still be used when appropriate. In many CPR classes, students continue to learn the traditional 30 compressions to 2 breaths method, along with AED use and other emergency steps.
The most important thing is not to stand there waiting. Start.
Better Use of AEDs
The 2025 guidelines continue to emphasize early AED use. An AED can check the heart rhythm and deliver a shock if one is needed.
This is why AED awareness matters in workplaces, schools, gyms, churches, airports, and public buildings. It is not enough to own an AED. People need to know where it is, how to get it quickly, and how to use it without hesitation.
A good CPR class should give students hands-on practice with an AED trainer so the device feels familiar instead of intimidating.
Dispatchers Are Part of the Rescue
A 911 dispatcher is often the first trained person involved in a cardiac arrest emergency.
The updated guidelines continue to support dispatcher-assisted CPR. Dispatchers can help callers recognize cardiac arrest, check for abnormal breathing, begin chest compressions, and locate an AED when one is nearby.
This matters because people often panic during an emergency. A calm dispatcher can help turn confusion into action.
CPR Quality Still Comes Down to the Basics
The 2025 guidelines continue to reinforce the same core CPR quality points:
Push hard. Push fast. Let the chest come all the way back up. Keep interruptions short. Use the AED as soon as possible.
These basics may sound simple, but they take practice. Most people do not naturally know how deep to press or how quickly to push. Hands-on training helps build that muscle memory.
That is especially important for healthcare workers, childcare staff, teachers, coaches, construction crews, manufacturing teams, and anyone expected to respond at work.
Updated Choking Response
One of the more noticeable 2025 updates involves choking care.
For a conscious adult or child with severe choking, the updated recommendation is to give 5 back blows followed by 5 abdominal thrusts, alternating until the object comes out or the person becomes unresponsive.
For infants, rescuers should use 5 back blows followed by 5 chest thrusts. Abdominal thrusts are not used on infants.
This is a good example of why staying current matters. Many people learned choking care years ago and may not realize the recommended sequence has changed.
Opioid Overdose Is Also Part of Emergency Response
The 2025 guidelines also place added attention on opioid-related emergencies.
If an opioid overdose is suspected, rescuers should call 911, check breathing, provide CPR if needed, and use naloxone if it is available. If the person becomes unresponsive and is not breathing normally, the situation should be treated as a life-threatening emergency.
This is becoming more relevant for schools, workplaces, public buildings, and community organizations that may now keep naloxone emergency kits onsite.
Communities Need More Than a Certificate
CPR certification is important, but the real goal is readiness.
A workplace may have people certified on paper, but do they know where the AED is? Does anyone know who calls 911? Can staff respond if the emergency happens in the breakroom, lobby, warehouse, playground, or parking lot?
The 2025 AHA guidelines continue to point toward stronger systems of care. That means training people, reviewing emergency plans, improving AED access, and making sure skills do not fade between certification cycles.
For healthcare settings, this is especially important. CPR and emergency response skills can decline over time, even before a two-year certification expires. Regular practice and refresher training help keep teams ready.
Why the 2025 Guidelines Matter
The American Heart Association updates its CPR and ECC guidelines as new research becomes available. The 2025 update builds on decades of resuscitation science and continues the focus on faster recognition, earlier CPR, quicker AED use, and better teamwork.
For the average person, the message is not complicated:
If someone collapses, do something.
Call 911. Start CPR. Get the AED. Follow the dispatcher’s instructions. Keep going until trained help takes over.
You do not need to be perfect to help save a life. But you do need to be willing to act.
Key Takeaways
Cardiac arrest remains a leading cause of death, and immediate action by bystanders can significantly impact survival rates.
The 2025 AHA Guidelines emphasize quick response, including calling 911, performing CPR, and using AEDs without hesitation.
Hands-Only CPR is recommended for untrained bystanders, while trained individuals should consider rescue breaths when appropriate.
The updated guidelines call for improved AED accessibility and training to ensure readiness in emergencies, including opioid overdoses.
Community preparedness goes beyond certification; it requires knowledge of emergency plans and continuous skill practice.
Each year, National Nurses Week is observed from May 6 through May 12, honoring the birth of Florence Nightingale and celebrating the compassion, professionalism, and commitment that define nursing. These values remain the foundation of modern healthcare.
Yet despite the respect and trust nurses earn, Florida continues to face a serious and growing nursing shortage.
State workforce data and nursing workforce studies show that more than 40 percent of Florida’s nurses are approaching retirement age. As experienced nurses leave the workforce, the demand for care continues to rise due to population growth, longer life expectancy, and increased healthcare needs. Without intervention, the shortage threatens access to care and places additional strain on hospitals, long-term care facilities, and outpatient clinics across the state.
Demand Is Outpacing the Supply of New Nurses
For anyone pursuing a nursing career in Florida, job opportunities are plentiful. While nursing school enrollment has increased nationally, it has not kept pace with projected demand.
This gap is not caused by a lack of interest. Nursing remains one of the most popular healthcare career paths, attracting thousands of qualified applicants each year. The challenge lies elsewhere.
Across the country, tens of thousands of qualified nursing applicants are turned away annually, not because they lack ability, but because nursing programs do not have the capacity to educate them. The primary reasons include:
In many nursing schools, faculty shortages alone prevent programs from expanding enrollment, even when student demand is high.
The Real Bottleneck: Nursing Educators
At the core of the nursing shortage is a shortage of nursing educators.
Many current nursing faculty members are nearing retirement, and fewer nurses are choosing academic careers. One reason is financial. Advanced practice and clinical roles often pay significantly more than teaching positions, making it difficult for colleges to compete.
As a result, schools struggle to hire and retain qualified instructors, limiting how many students they can accept and graduate.
What Prospective Nurses Can Do
While systemic change is needed, individuals interested in nursing can still take practical steps to enter the field sooner.
When researching nursing programs, consider the following:
Program Structure Does the program include all required coursework for licensure without lengthy pre-nursing delays?
Campus Availability Schools with multiple campuses or expanded cohorts often have shorter or no waiting lists.
Flexible Advanced Degrees If you are already a nurse, look for MSN programs designed for working professionals, including education or leadership tracks.
Transfer Policies Choose a program that accepts prior college credits so your previous coursework counts toward your degree.
Career Pathways Programs that support LPN-to-RN or bridge options allow students to enter the workforce sooner while continuing their education.
Transparent Costs Tuition should clearly include textbooks, lab fees, uniforms, and required materials so there are no surprises.
Choosing a Program You Can Start Now
Given the ongoing demand, it is important to explore nursing programs early and proactively. Some students choose to begin with practical nursing diplomas or associate degrees, gaining experience while working toward higher credentials.
Attending nursing information sessions, speaking with admissions counselors, and understanding waitlist policies can make the difference between starting now or waiting years.
Addressing the Educator Shortage
Long-term solutions must include policy and funding changes that make nursing education careers more attractive. Proposed solutions include:
• Competitive faculty salaries • Loan forgiveness for nurse educators • Funding for advanced nursing education • Expanded bridge and transition programs
Florida educators and technical schools have repeatedly called for legislation that supports career transition pathways, allowing licensed nurses to continue advancing their education and increasing the number of registered nurses statewide.
Moving Forward
The nursing shortage is not a distant problem. It is happening now, and Florida is on the front lines.
Whether you are considering a nursing career, already working in healthcare, or advocating for stronger education systems, being informed is the first step toward change. With thoughtful program selection, policy support, and long-term investment in educators, the cycle can be reversed.
One nurse can make a difference. Thousands can change the future of healthcare in Florida.
Here are reliable sources you can cite to support the updated article on the nursing shortage (focused on Florida and the national context). These sources include workforce projections, faculty shortages, and enrollment capacity challenges:
Florida-Specific Nursing Shortage Data
The Florida Center for Nursing reports ongoing demand for Registered Nurses in Florida, with a projected shortage of tens of thousands of RNs over the next decade as supply fails to keep pace with demand.
Florida lawmakers and health officials have highlighted a projected shortage of nearly 60,000 nurses in the next decade, citing workforce projections and gaps in nursing education capacity.
National Nursing and Faculty Shortage Data
The American Association of Colleges of Nursing (AACN) reports that U.S. nursing schools turned away more than 65,000 qualified applicants in 2023 due to insufficient faculty and other resource limitations, and that nursing faculty vacancy rates remain a challenge.
National data show nursing faculty shortages continue to limit enrollment capacity in nursing programs across the U.S., affecting the ability to educate enough new nurses.
Nationwide projections indicate that the nursing workforce supply is not keeping up with demand, with registered nurses remaining in shortage and openings continuing through 2034.
Additional Relevant Context
National workforce trend data show that nursing faculty—and healthcare workers generally—are aging and will contribute to ongoing workforce turnover, underscoring the importance of investments in nurse education and retention.
Updated by Troy Bowman 2026
Key Takeaways
National Nurses Week celebrates the nursing profession, yet Florida faces a severe nursing shortage due to high retirement rates and rising demand.
More than 40% of Florida’s nurses are nearing retirement, while nursing school enrollment does not keep pace with demand.
The nursing educator shortage exacerbates the problem, as many faculty are also nearing retirement and higher salaries in clinical roles attract nurses away from teaching.
Prospective nurses should explore flexible programs and transparent costs to begin their careers sooner, while addressing the educator shortage requires systemic changes.
Immediate action and informed choices can help mitigate the nursing shortage and improve healthcare access in Florida.
Mosquitoes can turn a relaxing evening outside into a miserable one fast. Their constant buzzing is irritating enough, but the itchy bites are what really ruin the fun. Most of the time, mosquito bites are more of an annoyance than a danger. Still, mosquitoes are not just harmless pests. They have been known to carry diseases, which is why prevention matters.
One of the best ways to avoid mosquito bites is to put a physical barrier between your skin and the bugs. In areas where mosquitoes are especially heavy, long sleeves, long pants, socks, and even gloves can make a big difference. Some hats also come with roll-down netting that protects your face and neck, which can be helpful in heavily wooded or swampy areas.
If you are camping, sleeping out under the open sky may sound peaceful, but it also makes you an easy target for mosquitoes and other biting insects. A sealed tent with fine mesh screening is a much better option if you want fresh air without spending the night getting eaten alive.
For people who do not want to cover every inch of skin, insect repellent is usually the next best line of defense. Products that contain DEET are still considered the most effective when used as directed. Apply repellent to exposed skin before heading outside, but avoid spraying areas that will be covered by clothing. You should also keep it away from your eyes, mouth, and fingertips, then wash it off once you come back indoors.
There are plenty of other products marketed as mosquito repellents, including essential oils, bracelets, and sound-based devices. Some people like them, but in general they have not performed nearly as well as DEET-based sprays in real-world use.
If you do get bitten, treatment is usually simple unless you are having a more serious allergic reaction. Oral antihistamines such as Benadryl may help. Topical treatments like anti-itch creams or benzocaine products are also commonly used. Many people also find relief from a cool shower or bath with mild soap.
Try not to scratch too much. As tempting as it is, broken skin can lead to irritation or infection, especially if you are outdoors, camping, or in less-than-clean conditions.
A few mosquito bites may seem like part of summer, but a little prevention goes a long way. With the right clothing, a good repellent, and a few simple precautions, you can spend more time enjoying the outdoors and less time swatting, scratching, and regretting every decision.
The latest research for 2026
Recent research is giving experts a better picture of why some people seem to be mosquito magnets. Scientists are paying closer attention to the role of the skin microbiome, because the bacteria on our skin help produce odors that attract mosquitoes. In one 2024 study, researchers even found that engineered skin bacteria made hosts less attractive to mosquitoes for an extended period, which hints at where future repellents may be headed. In the meantime, the most effective prevention is still much simpler: use an EPA-registered repellent with ingredients such as DEET, picaridin, IR3535, oil of lemon eucalyptus, PMD, or 2-undecanone, wear long sleeves when possible, and reduce standing water around the home where mosquitoes breed.
When bites happen, a few simple home remedies may help calm the itch. The American Academy of Dermatology recommends using an ice pack to reduce itching and swelling, and over-the-counter hydrocortisone cream or an oral antihistamine can also help. For a home remedy, Mayo Clinic notes that a baking soda and water paste may soothe irritated bites, and many people also get relief from a cool wash or bath. Whatever method you use, try not to scratch, since broken skin can raise the risk of irritation or infection.
CDC, Preventing Mosquito Bites Covers the currently recommended EPA-registered repellent ingredients, including DEET, picaridin, IR3535, oil of lemon eucalyptus, PMD, and 2-undecanone. CDC Yellow Book, Mosquitoes, Ticks, and Other Arthropods Supports current prevention guidance and repellent use details, including use considerations for children. PNAS Nexus, 2024 study on engineered skin microbiome Discusses research showing that engineered skin bacteria reduced mosquito attraction, which is part of the newer research angle. American Academy of Dermatology, Tips to Prevent and Treat Bug Bites Supports using ice packs, hydrocortisone cream, and oral antihistamines for itchy insect bites. Mayo Clinic, Mosquito Bites: Diagnosis and Treatment Supports the baking soda and water paste home remedy and other bite-soothing options
Aspirin has been a go-to item in medicine cabinets for years. Most people know it as something you take for pain, headaches, or fever. But for a long time, it was also commonly recommended as a daily step to help prevent heart attacks and strokes. That advice has changed.
Today, experts are taking a more careful approach. Aspirin can still play an important role in certain heart-related situations, especially during a suspected heart attack. But when it comes to taking aspirin every day to prevent a first heart attack or stroke, the guidance is no longer one-size-fits-all.
Why the advice changed
For years, many adults were told that taking a low-dose aspirin each day could help protect their heart. Newer research has shown that the decision is more complicated than that. While aspirin can reduce the risk of blood clots, it can also raise the risk of serious bleeding, including bleeding in the stomach or even the brain.
Because of that, health organizations such as the U.S. Preventive Services Task Force and the American Heart Association now recommend a more individualized approach.
What the current guidance says
For adults ages 40 to 59, daily aspirin may still be worth considering in some cases, especially for people with a higher risk of cardiovascular disease. Even then, the benefit is considered fairly small, so it should only be started after talking with a healthcare provider.
For adults age 60 and older, the recommendation has become more cautious. Experts generally advise against starting a daily aspirin routine for primary prevention in this age group, because the bleeding risk often outweighs the possible heart benefit.
For younger adults, especially men under 45 and women under 55 who do not have a history of cardiovascular disease, daily aspirin is usually not recommended as a preventive measure.
The safety concerns matter
Aspirin helps prevent clots by thinning the blood. That is also what makes it risky for some people. Regular use can increase the chance of gastrointestinal bleeding and hemorrhagic stroke. Over time, higher doses or long-term use may also create other health concerns.
When aspirin is used for prevention, lower doses such as 81 mg baby aspirin are generally preferred over full-strength doses. They can offer similar benefit with less risk. For everyday pain relief, many doctors may recommend other options depending on the person’s health history.
What has not changed: emergency use
One thing is still very important. If someone may be having a heart attack, aspirin can still be a lifesaving tool in an emergency. If 911 is called and emergency dispatchers advise it, chewing a full-strength aspirin may help while waiting for paramedics to arrive.
That does not mean people should self-prescribe daily aspirin. It means aspirin still has an important place in emergency response when used appropriately.
What this means for workplaces and training
These updates matter outside the doctor’s office too. If you manage workplace safety or First Aid supplies, it is important to understand the difference between emergency aspirin use and routine aspirin use. Aspirin may still belong in a properly managed First Aid setting for cardiac emergencies, but it should not be handed out casually as a general pain reliever.
It is also a good idea to stay current with First Aid and CPR training so your team understands the latest recommendations for responding to cardiovascular emergencies.
Disclaimer: Any aspirin dosage or preventive regimen must be discussed with a physician. Factors such as family history, current medications, and individual bleeding risks are essential to a safe health plan. Annual exams are highly recommended for anyone on continuous medication.
On any given day, nearly 62,000 injuries occur in and around the home in the United States. That breaks down to hundreds of injuries every minute—most of them minor, but many serious enough to require immediate attention. Cuts, bruises, and scrapes are common, but more dangerous incidents such as burns, poisonings, choking, and suffocation happen far more often than most people realize.
We tend to think of our homes as safe spaces—and they should be—but accidents don’t need much invitation. A wet floor, a hot stove, a loose rug, or a small object within a child’s reach can quickly turn an ordinary day into an emergency.
Where Household Injuries Happen Most
Even in well-maintained homes, certain areas naturally carry higher risk. Understanding where injuries happen is the first step toward preventing them.
Common injury zones in the home:
Kitchen: burns, cuts, fires, and food-related choking
Bathroom: slips, falls, and accidental poisoning (medications, cleaning supplies)
Living areas: trips, falls, and furniture-related injuries
Garage/basement: tool injuries, chemical exposure, and sharp objects
Yard/outdoor spaces: falls, equipment injuries, insect stings, and heat-related issues
👉 Most injuries are not caused by “unsafe homes,” but by unpredictable moments in familiar environments
Why Prevention Isn’t Enough
Safety-proofing your home—installing smoke detectors, securing cabinets, using non-slip mats—is important. But even the safest homes cannot eliminate risk entirely.
The real question becomes:
If something does happen… would you know what to do?
Would you know how to treat a severe burn?
Could you respond quickly to choking?
What if someone stopped breathing due to an allergic reaction?
These situations unfold fast, and waiting for help without taking action can make outcomes worse. In many cases, the difference between recovery and tragedy comes down to what happens in the first few minutes.
Common Household Injuries (Quick Chart)
Here’s a simple breakdown you can use visually on your site:
Most Frequent Household Injuries:
Cuts & lacerations → most common, usually minor but can involve heavy bleeding
Burns (thermal, electrical, chemical) → can escalate quickly without proper care
Falls → leading cause of serious injury, especially for children and older adults
Poisoning → often involves medications or household cleaners
In many household emergencies, time is the deciding factor.
Time is critical
Every second counts
Minutes matter
Delay = danger
What this represents:
As time without care increases, outcomes decline rapidly—severe bleeding, choking, and breathing emergencies can become life-threatening within minutes, but immediate first aid can stabilize the situation until EMS arrives.
In the event of a first aid emergency:
0–2 minutes: Quick action can stop bleeding, clear an airway, or remove a hazard before the situation worsens
2–5 minutes: Conditions like choking, severe allergic reactions, or heavy bleeding can rapidly become life-threatening
5–10 minutes: Lack of oxygen or continued blood loss can lead to serious injury, shock, or organ damage
10+ minutes: Risk of permanent damage or death increases significantly without intervention
First aid is not about replacing professional care—it’s about bridging the gap until help arrives
The Role of First Aid Training
Learning first aid equips you with practical, real-world skills that can be used immediately in an emergency. It allows you to take control of a situation rather than feeling helpless.
Recognize signs of serious conditions like shock or allergic reactions
Provide care that stabilizes a person until emergency responders arrive
Just as importantly, training builds confidence. In an emergency, people often hesitate—not because they don’t care, but because they’re unsure. First aid training replaces that uncertainty with clear action.
A Skill for the Entire Family
One of the most valuable aspects of first aid is that it’s not limited to professionals. It’s a skill that can be learned by anyone and shared within a household.
Families who learn first aid together create a safer environment for everyone. Children become more aware of risks, adults feel more prepared, and everyone gains the ability to respond when it matters most.
Training is also quick and accessible. Most courses can be completed in just a few hours and provide hands-on experience that sticks with you long after the class ends.
Staying Prepared Over Time
Like any skill, first aid should be refreshed periodically. Taking a refresher course every couple of years helps ensure that your knowledge stays current and that you can act quickly without second-guessing yourself.
It’s also important to:
Keep a well-stocked first aid kit easily accessible
Know emergency numbers and basic response steps
Review safety practices in your home regularly
Preparation doesn’t eliminate emergencies—but it changes how they end.
Final Thought
Accidents at home are common, but being unprepared doesn’t have to be. First aid training gives you the ability to respond, stabilize, and protect the people around you when something unexpected happens.
It’s a simple investment of time that can make an extraordinary difference.
For information about local first aid classes, visit inpulsecpr.com.
Love is one of the most powerful human emotions—especially the kind shared between a parent and child. Ask any mom or dad what they love most about being a parent, and you’ll see it instantly: a warm smile, followed by a list that could stretch a mile long.
Of course, there are also those unforgettable moments… like a quick trip to the store that turns into a full-blown meltdown because a ring-pop before nap time somehow feels like a perfectly reasonable request. Through every high and low, one truth remains steady:
“We wouldn’t trade them for the world.”
Every parent dreams about the future. The strong, hardworking man their son will become. The confident, accomplished woman their daughter will grow into. We do everything we can to guide them, teach them right from wrong, and protect them from a world that doesn’t always play fair.
Growing up looked different for many of us. Riding in the back of pickup trucks. No helmets. Streetlights were the only curfew we needed. Today, we wrap our kids in layers of protection—helmets, pads, supervision, safeguards. And that’s a good thing.
But when it comes to one of the most important forms of protection… many parents fall short.
When people think of CPR, they picture scenes from movies. “It’ll never happen to me.” “I’ve seen it on TV—I could figure it out.”
But real life doesn’t follow a script.
Life is fragile. It can change in an instant.
In 1995, I lost my son to SIDS (Sudden Infant Death Syndrome). There are no words strong enough to describe that kind of loss. As the saying goes, a parent should never have to bury their child. It’s a pain that reaches beyond anything physical—it settles deep and stays.
Some people never recover from that kind of grief. Others try to transform it into something meaningful.
For me, that moment came while watching the medics and firefighters work tirelessly to save my baby. Their determination, their skill, their refusal to give up—it left a permanent mark on me.
Years later, after a great deal of reflection, I made a decision: I went back to school and became an EMT.
Not long after, I found In-Pulse CPR. They were looking for instructors and assistants. It felt like everything had aligned—an opportunity to take something tragic and turn it into something that could help others.
I met Troy Bowman… and was hired on the spot.
Today, I help teach others a skill that I wish every parent truly understood.
A Simple Question Every Parent Should Answer
One of the first questions I ask new parents is:
“Are you certified in infant CPR?”
The most common response?
“I’m not certified, but I’m sure I could do it if I had to.”
That answer is more common than you’d think—and more dangerous than most realize.
CPR isn’t complicated, but it is specific. And those specifics matter.
What Many Parents Don’t Realize
Infant CPR is different from child and adult CPR
Proper hand placement and compression depth are critical
Timing, rhythm, and airway techniques must be learned—not guessed
In an emergency, there is no time to “figure it out”
Confidence comes from hands-on practice, not observation
In-Pulse CPR is built around one simple goal: helping people feel prepared when it matters most. Our team is dedicated to making sure you don’t just memorize steps—you understand what you’re doing and why it works.
Take a moment to look at upcoming classes. It’s a small investment of time… but one that could mean everything.
Because when it comes to the people we love most, “good enough” should never be the plan.
In-Pulse CPR is an American Heart Training Center leader. We are the largest and most respected provider of community based classes in the area. Learn to be an instructor from the best!
Why train with us? In-Pulse CPR has trained over 150 thousand students since 2009 . Our instructors are passionate about teaching and it shows. We have thousands of reviews from students on Google, Trustpilot and reviews.io that rave about our classes.
Do your research, you won’t find a better taught class in the state.
Please note: We limit our instructor classes to only 3 a year. Our next class is on:
American Heart Association AHA BLS Healthcare Provider Instructor Training HeartSaver CPR Instructor Certification
Equivalent Red Cross ARC CPR Instructor Classes
“Why would I want to be a CPR Instructor?”
5 reasons why you should Easier than you think – View the steps below Frequently asked questions
Starting a new career as a CPR instructor is affordable and can be very rewarding. The demand for more community taught classes is growing. You could help fill that need.
5 Reasons Why you should become a CPR Instructor
Work for yourself
Becoming an American Heart Instructor: You believe in the tremendous importance of CPR classes, and you have learned a lot by participating in these courses. If you are passionate about training and helping others, now is a great time to consider taking the next step and becoming an American Heart instructor. Once you complete your training, you’ll be able to take advantage of attractive benefits. Here are some of the reasons why becoming an American Heart instructor could be the perfect fit for you.
You can set your own schedule.
Flexibility is an important benefit to today’s job seekers, and working as a CPR instructor offers the schedule flexibility that you’ve been searching for. Once you are a certified instructor, you can choose the location, dates, and times of your classes. Teach classes on weekday evenings for busy parents, or schedule sessions during the day in corporate environments.
Get support and guidance from your Training Center
You can add impressive experience to your resume.
You want to give yourself every advantage in today’s competitive job market. If you are already working as a health professional, your current and potential employers will appreciate seeing the American Heart Instructor certification on your resume. This certification does not only mean that you are a CPR expert; it also shows that you have experience in teaching, speaking in front of a group, and instructing a class. Employers in a wide range of settings value these skills.
You set your own schedule
You can enjoy networking opportunities.
As we chat with those who are currently working as American Heart instructors, we find that many of them have made valuable connections through their classes. CPR certification is a requirement for all medical professionals, so you’ll have students from medical facilities throughout our local area. Whether you are looking for a new job now or sometime in the future, it’s helpful to have connections with medical professionals from a variety of specialties.
You can enjoy extra income.
Organizations ranging from schools to recreation departments realize the importance of providing quality CPR training for their employees. As they pay for these courses, you’ll be able to enjoy the benefit of extra income. Even if you only teach for part-time hours, you can earn additional funds for vacations, holiday gifts, and more.
You can make a life-changing difference.
We’ve saved the most important benefit of working as a CPR instructor for last. The process of teaching is rewarding, and it is even more so when the methods you are sharing can change lives. You’ll love seeing students leave your classes feeling empowered to act confidently in emergency situations. As your students go out into their families, work places, and communities, they have the power to save lives thanks to your careful instruction.
Steps Needed to Become a CPR Instructor
Instructor class are affordable
The steps are simple – get started today!
Approval to align with a local American Heart Training Center – The American Heart requires this. The good news is In-Pulse CPR is an AHA Training Center (TC) and is currently accepting instructor alignments in Florida.
Have a non-expired valid BLS and / or HeartSaver CPR certification before you attend an instructor class. Register Here! (Must be an American Heart certification)
Sign up, attend, and successfully complete the classroom Instructor Course. Call us at 813-343-4024 for information about our next class or visit the link at the top of this page to register online.
Successfully be monitored teaching your first course within six months of completing Instructor Course. Training Center Coordinators can require additional monitoring.
FAQ’s New CPR Instructors Ask
What does it cost to become an American Heart Instructor? A new instructor should be prepared to spend a minimum of about $900-$1200 to get started. As you grow, you can add to your inventory with more supplies and equipment as needed. The more equipment you have to teach with the larger your classes can be. A few of your startup costs include: -The Instructor course, alignment fee, and monitoring ($300-$500) -Manikins (a functional manikin can be purchased for around $160) Most instructors / teachers have multiple manikins. -AED trainers (start at about $120 each) -Additional training supplies and start up costs ($ varies) -Marketing / Website ($ varies) You may be able to help cut initial costs by finding used equipment to start out with.
Who do I train? Some people you might initially train are your family and friends, your church, or past employers. As you grow your business you may want to reach out to small to medium medical clinics, dental offices, daycares, and schools. There are thousands of people within your community who need this training. Many need CPR/ BLS training as a requirement for their job. This training needs to be completed every two years. BLS stands for ‘Basic Life Support’. It is often synonymous with CPR, more commonly refers to the medical side of CPR training that includes other life support functions like dealing with choking, assisted breathing, AED use, etc. As a BLS Instructor , you can teach healthcare CPR classes, as well as, laymen CPR (commonly known as HeartSaver CPR).
Where can I teach? Geographically speaking, you can teach anywhere. There are some restrictions on handing out a certification to someone outside the country though.
Once I take this class and start teaching CPR, who is my employer? This depends. Is an employer paying for your class and startup costs? Then they are probably your employer. If not, you are self employed. Being a self employed independent CPR instructor has many advantages. See 10 Benefits of Being Self-Employed.
Do I need a Healthcare background or public speaking experience to be a CPR instructor? The short answer is No, anyone can become a CPR instructor regardless of their background. That being said, having past experiences helps. If you are planning on teaching CPR to healthcare workers, it is hard to develop a rapport with your students if they have a medical background and you don’t. If you are only planning on teaching to non-healthcare students like that found at your church, warehouse staff, daycares, teachers, and similar, than a medical background is not important. Likewise, if you have public speaking experience and are an effective communicator, you may be skilled enough to establish a repour with many different types of audiences. Most new instructors have a few fears at first. The more often you teach, the more you can sharpen your communication skills and become a better instructor and communicator. The better you can connect with your students helps develop that trust your students are seeking. Having a good rapport with your students is huge; it is the difference with them giving you repeat business and passing referrals, to never doing business with you again.
When you attend an INSTRUCTOR CLASS with In-Pulse CPR, we will cover many of these questions within the course.
CPR and AED training are no longer something students might happen to learn along the way. In Minnesota, public school districts are required to provide one-time CPR and AED instruction for students in grades 7 through 12 as part of the curriculum. That requirement has been in place since the 2014-2015 school year, and the law specifically calls for a hands-on component, not just watching a video or hearing a lecture. Students do not have to earn a certification card to meet the school requirement, but they do need real instruction and practice.
That matters because students are often nearby when emergencies happen, whether at school, at home, at practice, or in public. CPR training gives them the confidence to step in during those first critical minutes before EMS arrives. A short, well-run class can teach students how to recognize cardiac arrest, start compressions, and use an AED. It is a practical skill, and in the right moment, it can mean the difference between waiting for help and becoming the help.
Why this matters right now
When a cardiac emergency happens, time matters. Survival from out-of-hospital cardiac arrest is still heavily tied to whether someone nearby starts CPR right away. The biggest problem is often hesitation. People freeze because they are afraid of doing it wrong or assume someone else will step in. Teaching CPR in schools helps close that gap by giving young people a skill they can carry for life.
Minnesota’s school-based CPR training law was built around that exact idea: make basic life-saving instruction a normal part of education instead of a specialized skill only a few people learn. It is one of the simplest ways to build a stronger emergency response culture in communities across the state.
What is changing in 2026
Minnesota lawmakers are also looking at expanding that same readiness to athletics. In the current legislative session, SF 3548 would require middle school and high school coaches and assistant coaches employed by a district or charter school to obtain and maintain CPR and AED training. As introduced, the bill says that requirement would begin in the 2027-2028 school year. So this is not yet a current statewide mandate for coaches, but it is a real proposal moving through the legislative process.
That proposal makes sense. Coaches and school staff are often the adults closest to student-athletes during intense physical activity, and they may be the first ones expected to respond if something goes wrong. Training them in CPR and AED use would strengthen the same safety net Minnesota has already started building for students.
How schools can meet the requirement
For schools, this does not have to be complicated. The law requires instruction, but it leaves room for districts to decide how to deliver it. Some schools bring in outside trainers for a single-day session. Others use a combination of classroom instruction, video-based learning, and hands-on practice with manikins. The key is making sure students get actual psychomotor practice rather than passive exposure.
As a local American Heart Association Training Center, we help Minnesota schools meet these requirements with flexible options that work around busy schedules. That can include on-site training, staff development, and full certification courses for students or employees who want more than the minimum required instruction.
FAQ
Is the school CPR requirement still in effect in 2026? Yes. Minnesota law still requires school districts to provide one-time CPR and AED instruction for students in grades 7 through 12.
Do students need certification to graduate? Not necessarily. The statute says schools must provide the instruction, but it also says the training does not need to result in CPR certification.
What about coaches? As of April 2026, coach CPR/AED training is the subject of pending legislation, not a final statewide requirement yet. The current bill would apply beginning with the 2027-2028 school year if enacted.
What is Minnesota’s Good Samaritan protection? Minnesota law includes Good Samaritan protections for people who provide emergency assistance in good faith at the scene of an emergency. The statute is part of Minnesota law on providing assistance in emergencies.
Fact: Confirms that since the 2014-15 school year, Minnesota public and charter schools must provide one-time CPR/AED instruction to students in grades 7–12.
2025/26 Amendment: Recently updated to explicitly include the Health and Safety Institute (HSI) as an approved curriculum provider alongside the AHA and Red Cross.
Fact: This bipartisan legislation, active as of March/April 2026, mandates that all high school and middle school athletic coaches and assistants must be trained and maintain current certification in CPR and AED use.
Context: The bill was authored by Senator Bonnie Westlin and received unanimous support from the Senate Education Policy Committee.
3. Medical Statistics and Survival Rates
Source:American Heart Association (AHA) 2026 Heart Disease and Stroke Statistics Update.
Fact: Out-of-hospital cardiac arrest (OHCA) survival remains a major challenge, but the AHA confirms that immediate bystander CPR can double or triple the chance of survival.
Source:AHA Newsroom (February 2026 Release): “CPR skills prepare communities to save lives when seconds matter.”
4. Local Workplace Compliance
Source:Minnesota Good Samaritan Law (Statute 604A.01).
Fact: Provides legal protection for bystanders (including students and coaches) who provide emergency assistance in good faith, which is a critical part of the educational curriculum for schools.
5. Student Involvement Data
Source:Minnesota State High School League (MSHSL) 2025-2026 Participation Report.
Fact: Cited in legislative testimony, showing that over 230,000 Minnesota students participate in sports, highlighting the impact of the new coaching mandate.
The 2025 adult BLS take-home messages reinforce that when ventilating an adult in cardiac arrest, rescuers should give enough tidal volume to produce visible chest rise while avoiding both hypoventilation and hyperventilation. The goal is controlled, effective ventilation rather than forceful or excessive breaths.
This point is easy to overlook, but it matters. Too much ventilation can be harmful, and too little ventilation can also reduce the quality of care. The AHA’s wording puts the focus back on practical observation: visible chest rise is the target, not oversized breaths or rushed bagging.
References American Heart Association. Part 7: Adult Basic Life Support.
The 2025 AHA guidelines more directly address disparities in lay rescuer CPR training and response. The recommendations call for targeted training and awareness efforts in racial and ethnic communities, low socioeconomic areas, and linguistically isolated populations. They also specifically recommend addressing barriers to performing CPR on women through education and public awareness.
This matters because survival is not just about the science of CPR. It is also about whether people are trained, confident, and willing to act. By naming these barriers directly, the AHA is signaling that improving survival requires both better technique and better public readiness across all communities.
References American Heart Association. Highlights of the 2025 AHA Guidelines for CPR and ECC.
Use of any advise on this site is purely at your own risk. The information supplied is designed to accompany CPR and first aid training not to replace. In-Pulse CPR, Inc disclaims any liability for losses you incur as a result of inaccuracy of the information provided on this website. Information on this site is for education, supplemental to examination by and advice of medical professionals. Any information regarding first aid treatments is not meant to replace the advice of medical professionals including physicians, paramedics, emergency room attendants, nurses or other licensed medical personnel.

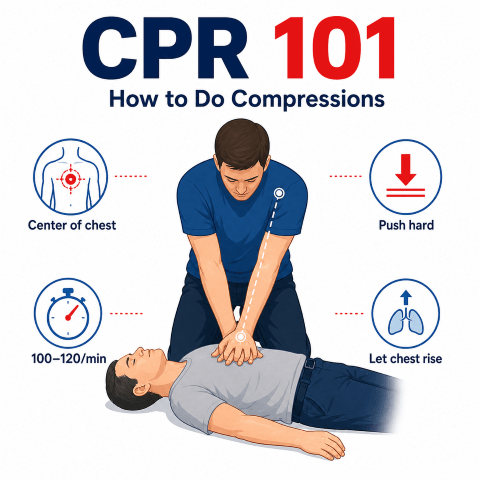
 by Troy Bowman
by Troy Bowman